The nature and structure of corporate social responsibility (CSR) make it difficult to include sectors that have long gestation periods and results that are not always quantifiable. Funds released annually under CSR need to be fully utilised within the year, there have to be impact assessment reports by external organisations within a certain time period, and projects have to lend themselves to clear, measurable outcomes.
Keeping the old, ailing and infirm in comfort and care, with adequate medical attention, through the last days of their lives does not tick any of those checkboxes.
Ajit and Sarah Isaac’s decision to focus on palliative and geriatric care as part of their personal philanthropic efforts, through the Thankamma Ithapiri Memorial Trust (TIMT) and the Ajit Isaac Foundation (AIF), had been influenced by their personal experiences. But the choice resulted in efforts being channelised towards a niche area of health care that is rarely covered by CSR.
“Two things influenced us as a family: One is all four of our parents had prolonged illnesses, and we realised that things like palliative care and geriatric care needed attention,” says Sarah Isaac, who grew up in Jamshedpur, where she became familiar with the health care infrastructure established by the Tata Group. “Around the time that my mother passed away, in 2016 of multiple myeloma, we discovered that end-of-life support in India is scarcely available. More than 13 to 14 million people need it in India, and less than 5 percent of them actually get it.”
They found that institutional investment in this area is not as much as it should be, and dignity of life, especially for those who simply can’t pay for it was difficult to find. “So it seemed a very obvious area for us to help, having seen what happened at home.”
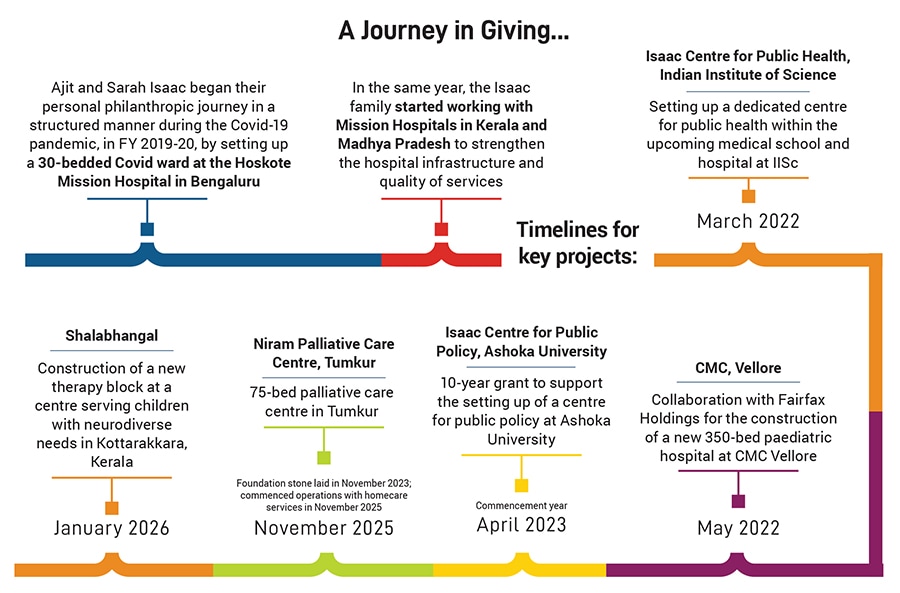
What these thoughts and efforts culminated into was the Niram Palliative Care Centre in Tumkur, Karnataka, which was inaugurated last October. In collaboration with the Rural India Mission Hospital, the centre operates a 75-bed facility that offers comprehensive care with terminal illnesses.
“It was about three years ago when the journey of getting into palliative care was started,” recalls Dr Naresh Shetty, project director, Niram Palliative Care Centre. “We were looking to start hospitals in remote areas, to make community health care available at all places. In large cities we have health care available at our doorstep, but when it comes to the remotest of areas, we do not have that.”
Their initial research and groundwork revealed that certain sections of the population were totally deprived of any health care, and that involved a lot of cancer patients. That was the first time they decided on whether to do something different from health care as a whole. “I said, why don’t we do only one thing, where we can help people in the last phase of their life? It’s not just about dignity in life, but also dignity in death. That was the starting point,” he adds.
It did not take much to convince Ajit and Sarah, who immediately recognised the need for palliative care in the country. “He said, we must do this because this is one area which is not at all developed in our country,” recalls Shetty, an orthopaedic surgeon who was president of the Ramaiah Memorial Hospital in Bengaluru for 28 years; the hospital has a pain and palliative care vertical for patients with terminal illnesses.
![]()
Palliative care is not restricted to cancer patients and is applicable to any chronic disorder, such as neurological conditions, paralysis, acute respiratory disorders, chronic renal disorders, or spinal injuries. One of the foremost challenges that Ajit, Sarah and Shetty noticed was that by the time patients required palliative care, they would have spent all their money on getting as much treatment as possible. The aim, therefore, became to provide care and counsel in order to make them feel better, but not charge them any money. “We will go back to the industry and find out ways and means to cover our recurring costs. Ajit covered all the initial costs, so that for the next two years the hospital runs on auto-mode and we can set up multiple such centers in Karnataka,” adds Shetty.
Ajit’s approach includes not just covering all the expenses of the hospital, but also a philosophical approach of ensuring that people are taken care of. Starting with one palliative care centre, the team aims to learn as many lessons as possible and then build on them. The team is foraying into home care, which includes an ambulance with a group of doctors and care workers who go to the homes of people in need. There are also plans to have a training centre very soon.
Ajit and Sarah’s efforts in the health care sector go well beyond the Niram Palliative Care Centre. “If you take health care as an overall sector, its reach in underserved regions, such as tribal areas, has not developed as much as it has in urban centers. Rather than a sectoral need in health care, there is actually a geographical need in health care,” says Ajit, founder and chairman, Quess Corp Limited. “For that reason we work with hospitals in a place called Chhatarpur in Madhya Pradesh, and another hospital in Nilambur, Kerala. These are slightly forested areas, and these are hospitals with 100 to 120 beds, between five and 10 doctors, and maybe two operation theaters that serve entire districts.”
![]()
AIF and TIMT has contributed to upgrading the infrastructure of Christian Hospital Chhatarpur, including adding an ICU, laboratory facilities, neonatal care capabilities, and advanced medical equipment. At the Burrows Memorial Christian Hospital in Alipur, Assam, AIF has helped set up an additional operation theatre with state-of-the-art equipment, while at the Marthoma Mission Hospital in Hoskote, Karnataka, TIMT provided 32 hospital beds, central oxygen supply, monitoring equipment, and more during the Covid-19 pandemic. At the Marthoma Mission Hospital in Chungathara, Kerala, TIMT and AIF have established an advanced ICU, NICU, operation theatre, and procured the essential medical equipment.
Paediatric health care is another area Ajit and Sarah decided to support, with the establishment of a multi-specialty paediatric hospital at Christian Medical College, Vellore. “The quality of work is outstanding; their medical care is perhaps the best available in India,” says Ajit. “The research they do is substantial, and they have built a fantastic track record of supporting sick people. So when they were building a pediatric hospital, it was an automatic choice for us to support that.” The 400-bed hospital is expected to be up and running by about October this year.![]()
Ajit Isaac (centre, in black shirt) with the team of Isaac Centre for Public Health in front of the centre’s building, which is under construction on the Indian Institute of Science campus in Bengaluru. Photo courtesy Ajit Isaac Foundation
AIF is also partnering with Johns Hopkins University in the US to develop a geriatric care centre in Koramangala, Bengaluru. “So, if you notice, it’s at the two different ends of an individual’s life—at the beginning and at the end—that we are getting involved with, not quite as much by design, but by the experiences that we’ve had, by the people we’ve met, and by the institutions that we’ve been able to partner with,” says Ajit.
Ajit and Sarah’s personal philanthropic work—as distinct from the CSR initiatives of Quess Corp—support areas that otherwise do not find support very easily. “That’s a core responsibility that we have, as a family philanthropic foundation; we have the responsibility to support very high-need yet niche areas. This governs how we pick up causes, identify high-need areas that are not often supported by, say, a typical, institutional large CSR mandate because of multiple reasons,” says Sweety Thomas, CEO, AIF.
![]()
The second factor that influences the choice of causes to support is the idea of backing people who understand their work very well and need the enabling support of a foundation. “In most of these cases, we come in at the initial level of the project or at seed stage, which is again very oriented to being social risk capital for any of these ideas. We come in when the idea is just germinating and we see it through,” explains Thomas.
Consequently, AIF does not have very stringent, thematic focus areas; it is more of an approach. One is to build institutions that can, in the long run, be exemplars in their areas of work—which is what it is trying to do by setting up the Isaac Centre for Public Health at IISc, Bengaluru, and the Isaac Centre for Public Policy at Ashoka University—and the second is to support high-need causes that may otherwise not find much support.
Elaborating on the first point, Thomas says AIF’s biggest involvement is its association with Ashoka University, with the Isaac Centre for Public Policy, which focuses on advising and working with governments, whether state or central, at creating better policy, whether it is for employment, economic reforms, agriculture, or health. Its public policy related work covers research, which includes working as technical partners with state and central governments, and running an academic programme for students who want to be trained in public policy, because the Centre invests within a university.
![]()
The other aspect focuses on law and legal reform. “One of our partners is an organisation called Vidhi Legal, which works on looking at existing laws and advising lawmakers as well as governments as to how these can be improved,” says Thomas. “We worked with Vidhi on one core project on decriminalisation. There are a lot of archaic, British laws that we still have, which have criminal repercussions when they shouldn’t. Vidhi works on these to see which of these can become more non-punitive from the point of view of attracting jail terms.” The impact of this is to increase the effectiveness of the judiciary and better turnover within courts wherein cases get resolved faster.
Thomas highlights how despite the lack of any compulsion on the Isaac family to give money towards personal philanthropy, they are choosing to give. “They are very, very invested in giving it very meaningfully because no one gives this quantum of money and doesn’t want to know that it is being used well,” she says, adding that Ajit sits on advisory boards of all the large grants for the Niram Palliative Care Centre because it was in-house; they have been involved in all the staffing decisions, all the construction decisions, all the major strategic outreach decisions.
The fact that the AIF team sits out of the corporate office in Bengaluru means there is very close access and interaction on the day-to-day affairs of the foundations, with Ajit and Sarah stepping in wherever they are required. Thomas points to the commitment that both Ajit and Sarah have towards the work that the foundation does, and to the fact that their daughter Tanya, who holds a PhD in public health from the Mailman School of Public Health at Columbia University, is very well qualified to give technical inputs as well.![]()
Ajit Isaac at the launch of the Isaac Centre for Public Policy at Ashoka University. Photo courtesy Ajit Isaac Foundation
“The foundation has their name on it, not someone else’s. At the end of the day, it is so much about their goodwill, their own brand equity, for lack of a better word,” says Thomas. “But that’s not what drives their involvement. The involvement is from the mandate that if we are choosing to give and give a substantial part of our wealth, it has to be meaningful and it has to be money-plus-sweat; it’s not either or.”
Ajit reiterates that for Sarah and him, giving economic resources is only one part of the story, and that the major part of what they do is the identification of the area they want to participate in and the institutions they want to partner with. There are certain criteria they have with regards to the institutions they want to partner with. He points to the fact that AIF and TIMT have teamed up with the best institutes and organisations in order to bring real impact to the chosen field of work.
“If you look at all the institutes we’ve partnered with, for paediatrics it is CMC Vellore, for public health it is with IISc, for public policy it is with Ashoka University, and for palliative care our association is with Johns Hopkins, for judicial reform we work with Vidhi,” he says. “So, we tend to go with track records, the people leading them, the kind of investments they have made in it. Other than the commitment of financial resources, we help them with networks and finding people for themselves. All these organisations, like any other organisations, go through phases when they need thought and support, when they need to be able to fall back on people with a vested interest to be able to find a path forward.”
At the end of the day, what makes all of this worth it for Ajit and Sarah are not the prestigious associations, and large cheques, and projects bearing their names, but the small moments in which they learn how all of it affects the lives of common folks in some of the remotest areas of the country.
“A couple of years ago I was at Nilambur, where the local MLA sought me out and said that earlier it was difficult for them to go to cities to look for health care, with women giving birth at home, road accident victims finding it difficult to get to doctors on time, get treatment or surgery,” remembers Ajit. “He was absolutely thankful that a remote place like Nilambur, which grows the country’s best teak and has India’s only teak museum, now has a small hospital, which we support, almost in the middle of nowhere.”