If we cannot solve vaccine equity globally, we cannot escape variants locally: B
Living through the pandemic has taught us some valuable lessons about how to live through uncertainty and prepare for it, the professor of biostatistics, University of Michigan School of Public Health
With waning immunity and breakthroughs, a large number of infections can happen quickly and even a small fraction of that needing hospital admissions is going to crumble the fragile health care systemImage: Danish Siddiqui/ Reuters
Advertisement
In the last two years I, like many of my friends, have lived, breathed, and sighed on the epidemiology of Sars-Cov-2. When our team started modeling the trajectory of this insidious virus in India in March 2020, none of us expected the pandemic to last this long. We ended 2020 on an optimistic note, with multiple vaccines showing promising efficacy results in clinical trials and receiving emergency use authorisations. The rollout of the vaccines brought tears of joy to millions of eyes as we welcomed 2021. Those moments will always represent the triumph of science and humanity to me. However, after this uber-uncertain vaccine-versus-variant roller-coaster of 2021, first Delta and then Omicron, we have learned some key lessons as we embark on the journey in 2022. Here are my top five lessons from 2021, followed by a summary of what I think 2022 may bring for
(1) We need global collaboration to end this pandemic it is a synchronised relay race of the whole world together, if there is something like relay marathon. No country can possibly get ahead of the other, there is no quick solitary win here. If we cannot solve the issue of vaccine equity globally, we cannot escape the variants locally. A colleague of mine aptly said if we replace the “I" in illness by “we", it becomes wellness. In this time of contagion, our own potential outcome does affect the outcome of others. Due to this spillover effect, we must make individual sacrifices for the collective good.
(2) The need for robust and transparent public health data systems and large cohorts with integrated data. Many of the key papers on Covid have come out of the UK, Israel and Denmark due to their national health/insurance systems database or population-based cohorts. Integrating testing, vaccination, sequencing databases with clinical data were key to identifying new variants and characterising their immune escape, transmissibility, and lethality properties. These multi-platform, cross-talking databases also gave us real-time data on vaccines and their effectiveness.
In the early days of Covid, they primed us about who is at the highest risk of hospitalisation due to Covid. When I started working on the India data, the data-paucity was eye opening. It is nearly impossible to find national level age-sex disaggregated counts on Covid deaths. Many deaths get unregistered, undercounted. After two years of Covid I am yet to see the daily hospitalisation data across India. Some data sources exist on governmental websites, but it takes incredible amount of effort to web-scrape and collate them in a usable format for running models.
My conclusion is that we have many excellent mathematical and statistical models on Covid, but very few countries have had reliable and accessible data to inform/train those models. It is time to invest in such systems as this is certainly not the last public health crisis the world is going to face. A robust data system bolstered by data transparency can evoke public confidence and trust in policies. Data denial and data opacity do not help, even the government.
(3) Embracing the notion of uncertainty and the humility of incomplete knowledge. To adequately model Covid we needed a model for virus transmission, a model for virus mutation, a model for public health interventions and their effects, a model for vaccine escalation and effectiveness, and finally a model for human behaviour. Identifying different components of these models and tying them together is nearly impossible. Thus, whatever we predicted was only tenable for the short term. Long-term, wide-ranging predictions were meaningless. Even within a 30-day horizon, one had to be modest about how ittle we knew and how rapidly things on the ground could change. The same thing about life: Decisions needed to change overnight about a trip, a gathering, or a classroom lecture. Elasticity and adaptability are key here.
(4) Public engagement, scientific communication, and pace of research: Harnessing the information tsunami to identify and deliver key messages was challenging, even for scientists. As modelers we are used to working behind the scenes. To be in the public eye was a huge leap for me, but many did this very successfully. The rapid pace of research and the urgency to influence/guide policy meant seeking alternative modes of communication and often settling for a “good" analysis as opposed to an “ideal" analysis. It led to not just writing peer-reviewed papers, but using social media, newspaper articles, blogs, and Medium articles. Scientists had an opportunity to directly engage with the public in real time. This is a completely different format of communication than what we are used to. The trolling and politicisation were also something new. For example, when I first started talking about the degree of undetected infections and deaths in India, I was highly criticised, but months later data came in from seroprevalence surveys and excess death studies that substantiated the model assertions. Similarly, when many were predicting a third wave in the Fall of 2021, our models never did, and I had to go on television and say that. You must nuance your messages here, as such predictions can also induce a false sense of security and lead to relaxed adherence to public health measures. Sticking to scientific truth is crucial.
(5) Striking a balance: Throughout this pandemic, we have struggled with charting a path that strikes a balance between alarmism and denial. Even now, some are proclaiming a cataclysmic Omicron wave while others are saying Omicron is clinically mild and will lead us to endemicity without causing a spike in deaths. There have been so many Covid curve balls thrown at us, a middle road is extremely important to define, for individual decision-making and for public policy.
Some scientists proclaimed by the end of 2021 that Covid will be endemic, like flu, and that was premature and unwise. Millions of people worldwide are dealing with long Covid, many countries in Africa have a less than 20 percent vaccination rate, almost no country in the world has a high degree of population with booster doses (which seems to be the only thing working to offer a reasonable level of protection against Omicron). The situation after two years of intense and arduous fight is still quite bleak. Our reservoir of hope, resilience and grit is depleting over time. However, we must think about joy and mental health and find a way to live with Covid.
I personally am trying to adapt to a dial-up, dial-down modality of life in concert with the virus incidence curve. This disrupts our regular rhythm and pattern of life, but we must evolve and accept the randomness of this bizarre period. We must also grieve and recognise our loss instead of being in a mad rush to get over the pandemic. The second wave in India had led to so many untimely deaths, we need to heal as a country. For me, as an immigrant scientist, sitting here in the US, watching my family suffer through Covid in India was painful and every day I process that trauma of last summer and try to contribute to the fight against Covid.
As I try to wrap my thoughts around Covid 2022, the one thing that is for certain is that it is not over. The immune escape properties of Omicron are making me very nervous about India. The high degree of past natural infections, combined with vaccination has been protecting India in late 2021, but if you consider the peak timing of past infections in April-May 2021 and the fact that almost no one has booster doses yet, the predictions for next year are bleak. It is key to know how many people have had “three hits": One infection and two vaccines to arrive at an accurate prediction. With waning immunity and breakthroughs, a very large number of infections can happen quickly and even a small fraction of that needing hospital admissions is going to crumble the fragile health care system. So instead of being complacent and feeling exceptional, we should plan for the worst and scale up health care resources, including new treatments for Covid so that we face the Omicron wave as best as we can.
This is not the last variant this is not the last pandemic. We should closely track hospital admissions and take stringent measures if the capacity runs the risk of being full. Quality masks and rapid tests should become common practices at gatherings. As a statistician I feel we need to do more work in quantifying the effect of interventions that were rolled out in bundles through worldwide natural experiments. What works and what does not work for India, for example, enforcing social distancing is hard but perhaps high-quality masks are not hard to distribute and mandated in indoor spaces. We need to think about boosters, scale up vaccine acquisition so that both first and second dose vaccination and boosting can continue in parallel. We must be nimble and transparent with data so that cluster infections, breakthroughs and new variants can be identified quickly and shared
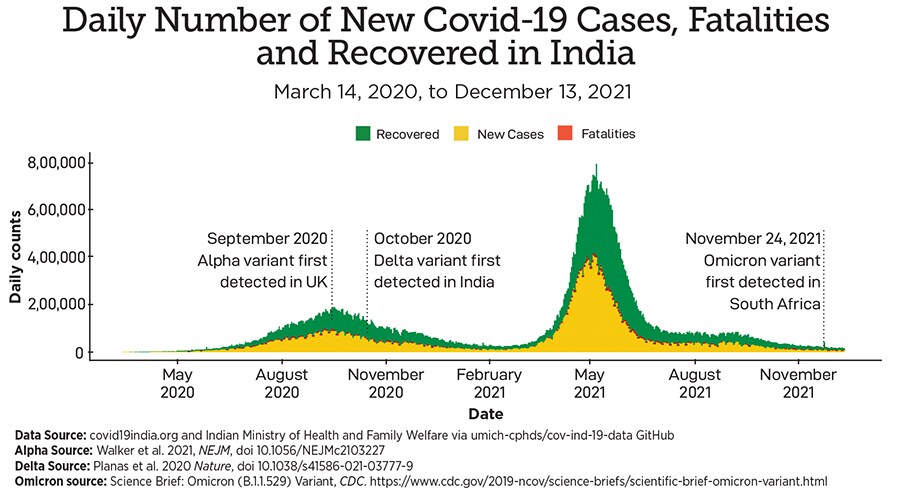
The following curve reminds us that we never know sitting in the valley of the curve when the next tidal wave is going to crush us. In the long run, my prediction is that we will likely have to go through cycles of boosters every six months until the world gets vaccinated/boosted. Endemic equilibrium is not in sight until global vaccine equity becomes a core value that everyone assents to. Till then, may science, solidarity and truth prevail in the face of adversarial uncertainty and political pandemonium.
The writer is professor of biostatistics, University of Michigan School of Public Health